| Common Signs & Symptoms | |||||
| Pain | Swelling | Stiffness | Weakness | Instability | Locking |
The Injury
A broken ankle is a common injury – there are over 250,000 each year in the United States alone. A broken ankle may occur as a result of direct contact, such as a road traffic accident or a sports opponent, but broken ankles are usually the result of a fall where the ankle twists under the weight of the body. Commonly tripping on a step or curb can be a mechanism for injury. There are numerous types of ankle fracture, classified according to the location of the fracture lines. To understand the nature of a broken ankle and how they occur, it is helpful to have a basic knowledge of ankle anatomy.
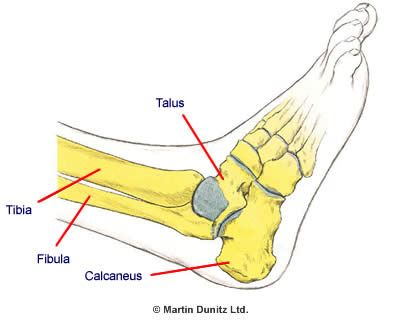
The ankle is made up of three bones – the Tibia (shin bone), the Fibula (splint bone) and the Talus, which are bound together by strong ligaments. The lower part of the shin bone and Fibula have bony prominences called the Medial Malleolus (shin bone) and Lateral Malleolus (splint bone) which form a ring around the Talus bone, which is referred to as the ‘ankle mortise’. The Talus is held in place by the anatomy of the surrounding bones and ligaments and any break in the bones that results in a disruption of the stability of the Talus is classed as an ankle fracture.
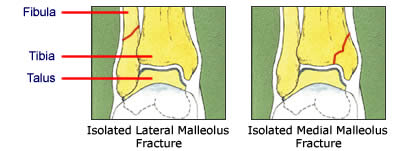
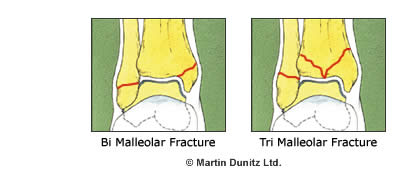
Ankle fractures are named depending on the exact location of the fracture line. Lateral Malleolus and Medial Malleolus fractures can occur in isolation or together (Bi-Malleolar fracture), or with fractures of the back of the Tibia (Tri-Malleolar fractures).
Signs & Symptoms
There is typically a history of twisting or trauma accompanied by a great deal of ankle pain and an inability to use the affected ankle. Any suspected broken ankle needs to be urgently transferred to hospital for assessment by a specialist trauma doctor. ‘Open’ fractures, where the bone fragments push through the skin, are blatantly obvious but all serious ankle injuries require a full assessment and an x-ray evaluation.
Treatment
What you can do
| Consult a sports injury expert | |
| Protect the ankle with a removable plastic cast | |
| Wear an ankle support for protection | |
| Use a wobble board to improve proprioception | |
| Use a buoyancy aid for pool fitness exercises | |
| Use massage to help reduce swelling | |
| Use resistance bands to strengthen the ankle | |
| Use a bone healing system to speed up broken bone healing |
The orthopaedic doctor will evaluate how the injury occurred and formulate a plan to restore normal ankle alignment. The ankle is reviewed with an x-ray and CT scan as the bones must be re-set within millimetres of normal position to prevent the later development of ankle arthritis. A broken ankle and any associated ankle dislocation must be ‘reduced’ to its normal anatomical position as early as possible to prevent nerve damage, damage to the blood supply or damage to the skin around the fracture.
If there is only one break of the ring of the ankle mortise, such as an isolated Lateral Malleolus or Medial Malleolus fracture, then non surgical treatment with immobilisation is usually sufficient. If required, the ankle fracture is put back into place by an orthopaedic doctor with the patient under a general anaesthetic. The orthopaedic doctor will review the ankle joint alignment after 48 hours, then again after a week or two weeks because the ankle alignment can be lost as the ankle swelling resolves.
The patient will have a plaster cast for two to three weeks and will be unable to weight bear. After three weeks if there is no pain and the x-rays show that there is good alignment then the patient can use a Removable Plastic Cast Walker. These are much lighter and more comfortable than a plaster cast and allow controlled weight bearing as well as re-introduction of functional movements, which actually helps the fracture to heal better. A broken ankle treated with immobilisation will take between 12 and 16 weeks to fully heal.
A double break (Bi-Malleolar fracture), or more complicated break of the ankle (Tri-Malleolar fracture), will require surgical fixation using screws, pins or plates to restore the normal ankle anatomy. If the ankle fracture or ankle dislocation is ‘open’ – i.e. the fragments are sticking out through the skin – then the wound must be surgically irrigated as soon as possible and monitored to prevent infection. If the joint surfaces of the Talus, Tibia or Fibula bones are damaged by the fracture then they must be meticulously realigned to reduce the risk of developing ankle arthritis. Research has shown that the outcome from ankle fracture surgery is better if the surgery takes place within three weeks of the injury occurring.
There are several possible complications that can occur following a broken ankle. ‘Fracture malunion’ can occur when the fracture fragments move and the fracture doesn’t heal in the correct position. This causes poor alignment of the ankle bones and eventually this causes ankle pain and arthritis.
‘Non union’ is a complication following a broken bone, where the bone fragments fail to heal sufficiently. Non union can be common following Medial Malleolus fractures that are treated conservatively. It may not cause pain, but it prevents a return to full function. Surgery may be required to fix a non union together.
The key principle of ankle fracture rehabilitation is to maintain the restored anatomy of the ankle joint, while restoring full range of ankle motion as early as possible. Walking as soon as the orthopaedic doctor indicates that it is safe to do so using a Removable Plastic Cast Walker is also important to encourage normal movement. This prevents complications such as muscle wastage, joint stiffness and degeneration of joint cartilage. By putting a carefully controlled load through the injured ankle it also stimulates fracture healing and helps to prevent non union.
The orthopaedic doctor will give permission to start bearing weight on the ankle to pain tolerance. This is graduated from partial weight-bearing with a Removable Plastic Cast Walker and crutches to full weight-bearing without crutches. A physiotherapist will encourage a normal walking pattern without any limping. Ankle swelling is common following a broken ankle. Massage and elevating the affected ankle while resting can be extremely effective at resolving a swollen ankle.
The compression provided by the Removable Plastic Cast Walker also encourages the dispersal of ankle swelling. The inflatable air cells of the Removable Plastic Cast Walker have a massaging effect during walking, which helps to resolve swelling. A plastic cast walker offers the added advantage of maintaining general fitness by enabling the use of a static exercise bike and resistance weight machines in a gym.
Ankle pumping exercises are excellent for restoring ankle range of motion and these can be progressed to Exercise Band resistance exercises to build strength around the ankle. Starting with a light resistance repetitions of inversion, eversion, plantarflexion and dorsiflexion should be started to regain strength lost through immobilisation. If the exercises are pain free, the strength of exercise band can be gradually increased depending on pain. Seek advice of a Physiotherapist in order to safely progress rehabilitation after an ankle fracture and ensure you don’t do too much too soon. Use pain as a guide as range of movement and strength exercises are introduced.
Once muscle strength, ankle joint motion and proprioception abilities are equal to the unaffected side, then a progression of functional training, such as running and sport specific drills can be started under the supervision of a Chartered Physiotherapist. Many people find that wearing an Ankle Support is reassuring when returning to sports training.
Prevention
Unfortunately, there is not much that can be done to prevent a broken ankle. In football it is important to wear ankle guards or ankle pads at all times in order to reduce the risk of a broken ankle from contact. Proprioceptive and strength training can be effective in reducing excessive twisting that could lead to injury. Physiotherapists can prescribe exercises and drills to include in a pre-habilitation programme.